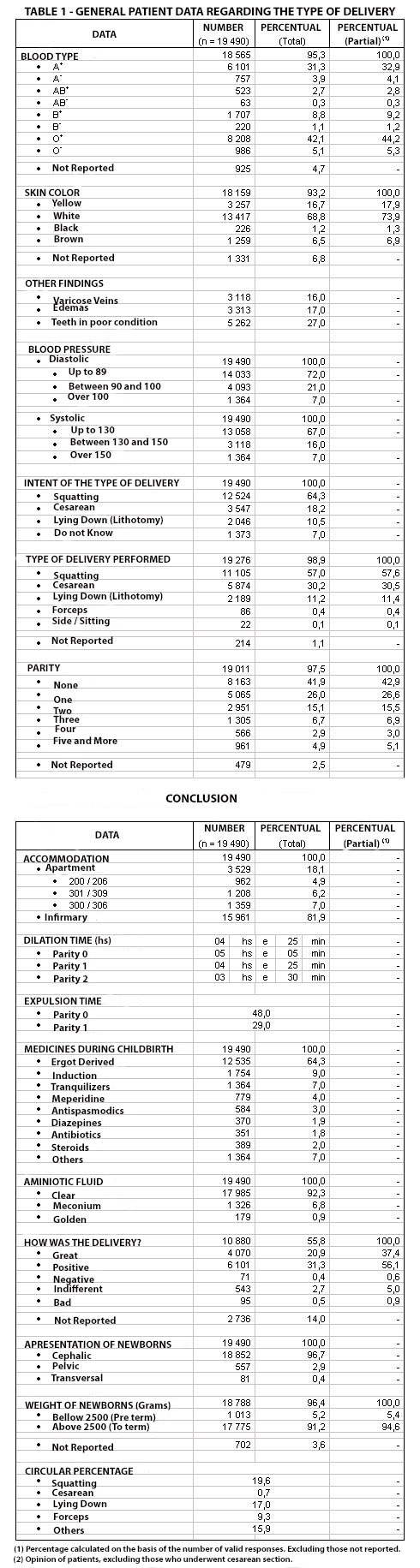
Of Labor
Although we have put side by side different data and classified them by type of delivery, we do not intend at this point of the study to establish definite conclusions on what is better, but show what has happened.
Labor total time considering it from 4 centimeters dilatation to the placenta delivery was 6 hours (average) for primiparous patients.
First Stage
Patient’s free ambulation was stimulated since the beginning of the work. Such procedure was spreaded to every case. The antepartum room, including its routine of analgesic for the primiparous was abandoned. When we tried – due to a require for comparing positions delivery – to gather a pregnant group which would lay, the patients refused vigorously.
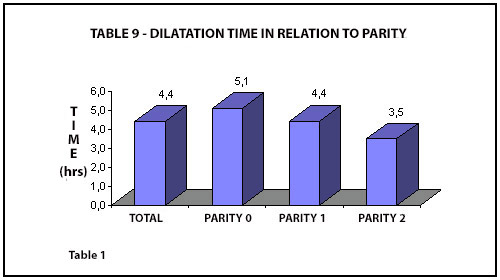
The cervix dilatation average time was DT = 4h25min. And into parities: For 0 – DT = 5h05min / For 1 – DT = 4h25min / For 2 – DT = 3h30min.
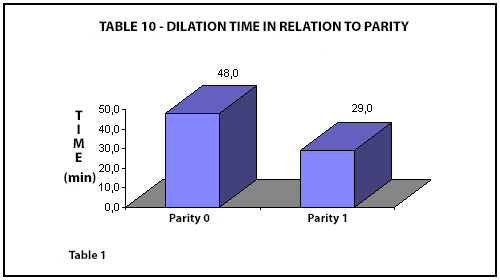
Second Stage
Watching the figures, we seen an average expulsion time for 0 – ET = 48 minutes with a slight difference favoring squatting position. We repeat that we are not pointing out significant differences favoring squatting position delivery since the group was spontaneous.
From the clinical point of view what is observed during second stage is that patients in the squatting position have less frequent contractions and a bigger control of the push which grows naturally.
Placenta Delivery
Average time for placenta delivery was 19 minutes for squatting position delivery and 15 minutes for supine position delivery.
Also from the clinical point of view: the placenta is expelled spontaneously without need for obstetrician maneuvers in the squatting position delivery. Another possibility is the conscious expelling of the placenta when the patient squats.
Placenta retention occurred in 0,3% of the cases without distinction between types of delivery position.
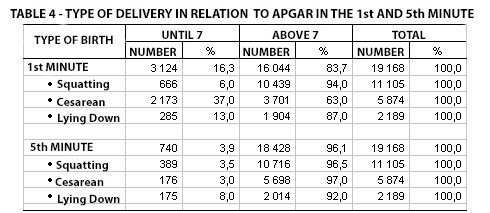
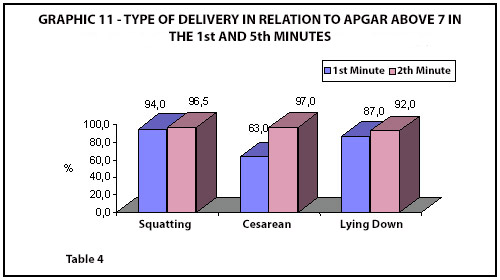
Apgar Score
For vertical delivery positions it was, in 94% of the cases over 7 in the first minute, and in 96,5% over 7 at 5 minutes. For supine position, 87% over 7 in the first minute and 92% over 7 at 5 minutes. For C-section, 63% over 7 in the first minute and 97% over 7 at 5 minutes.
Bruck and Ceccato – neuropediatricians and neonatologists, examining 346 children born through the squatting position, 62 through supine position, and 92 through C-section found an evident difference by the birth moment concerning the Apgar score at the first minute of the newborns through C-section. In the vaginal delivery they did not see any significate difference. These deliveries presented more retinian hemorrhage cases than the surgical deliveries. They followed those children’s growth for 5 years (1981/1986) and concluded that no significant differences occurred to the neuropediatric exam and the growth exam.
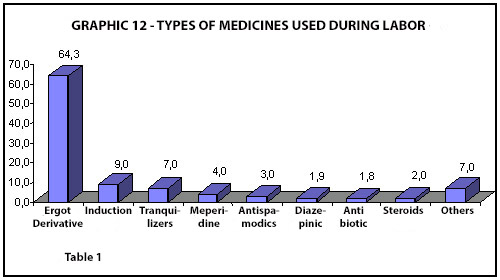
Medicines Used During Delivery
The only routine medicine used in the squatting position deliveries was a by-product of the ergot which is being revised today due to mother’s stimulation for keeping contact with their children and breastfeeding right after the birth.
Tranquilizers were used in 7% of the cases, the meperidine in 4%, and the antispasmodic in 3%. Labor induction occurred in 9% of the cases.
Epidural anesthesia was used as routine for C-section and in 80 cases of non-surgical deliveries.
Amniotic Membranes and Fluid
Membrane artificial rupture occurred as exception. In 5% of the cases it was unruptured in the delivery moment, in 2% it was artificially provoked, and in the other cases it happened spontaneously.
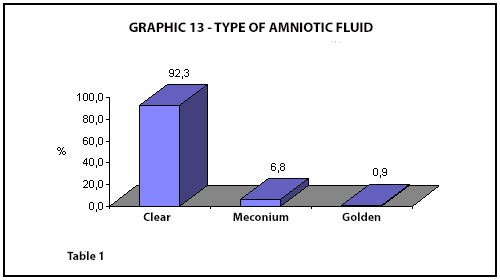
Meconium appeared in 1.326 cases, goldish yellow fluid in 179 cases. Establishing a relationship between meconium and Apgar score at the first and fifth minutes it becomes evident that most part of the population’s score is over 6. Thereof, this clinical datum, unquestionably an alert datum, must be evaluated together with other data, and does not justify, by itself, the occurrence of interventions.
Complications and Bleedings
We divided bleedings in moderate, abundant and excessive. There has been no difference between squatting and supine position delivery. In both groups the bleeding was mostly moderate.
For abundant and for excessive there has been predominance of forceps delivery.
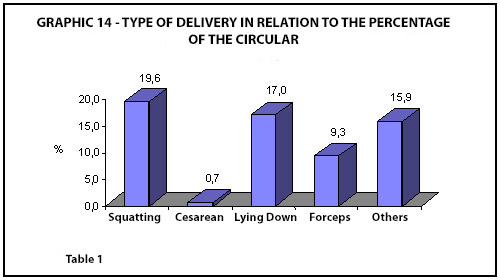
Circular of Umbilical Cord
It happened in 19% of the deliveries with no significant difference between squatting and supine position. In C-sections it has not been computed.
Perineum Aspects After Delivery
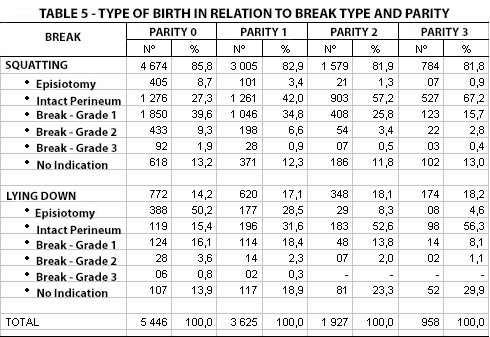
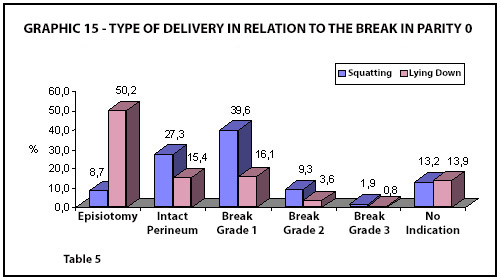
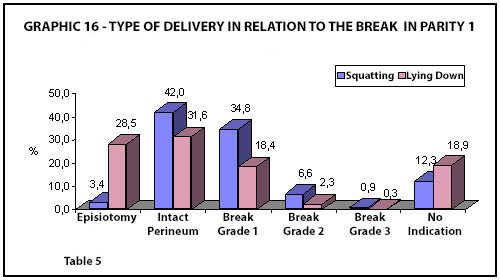
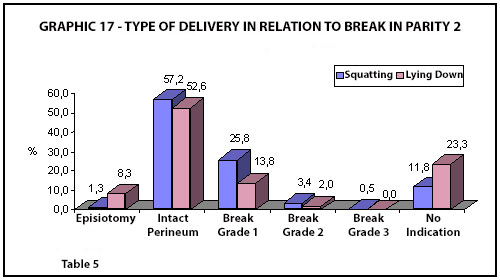
The graphs bellow demonstrates the perineal aspect after delivery:
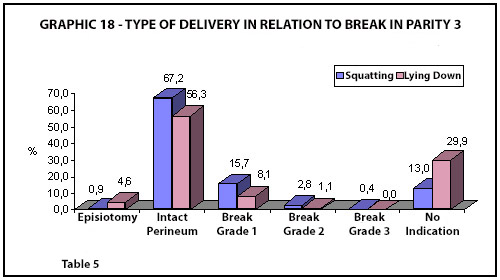
Discussion
I would divide in two parts the perineum aspect matter. The first is about the routine episiotomy: we can see in the above table that 27% of the for 0 have no tear at all after the delivery, as well as 42% of the for 1. First grade tear occurs to 40% of the for 0 and 35% of the for 1 population. We would consider episiotomy, as for its extension, second grade. That is, its routine application is wider than what happens to 69% of the patients. It would be advantageous to the 2% of the patients who present 3rd grade and it would be equivalent to the 9% who present 2nd grade tear.
From the clinical point of view, in some cases episiotomy, due to its surgical incision, makes episiorraphy easier. However, bleedings due to incisions are more abundant. Since we consider important to stimulate breastfeeding right after the delivery, which happens before placenta delivery and revision, the advantage gets minimized.
My conclusion is that routine episiotomy is not advantageous for the patients and it shall be done with more accurate indications.
Watching the graphics of the patients who had their children in the supine position we see that 50% of the for 0 had surgical incision of the perineum, and ruptures happened as follows: 16% first grade, 4% second grade, and 1% third grade. For 1 the figures are: 29% episiotomy, 18% first grade tear, 2% second grade, and there have been 2 cases in 620 of third grade tear.
And now the second part of the discussion which is a question: what delivery position protects more the perineum? To be able to answer it would be necessary not to perform episiotomy in a great number of patients who have supine position delivery and then compare the results.
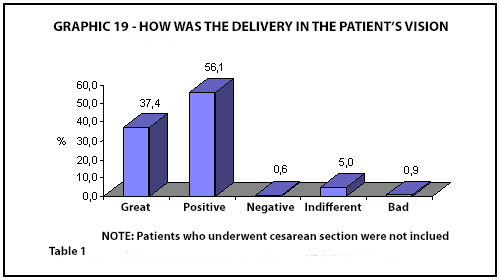
Delivery for the Mother
That question has been asked to the patients right after revision was done, before they left the delivery room. Here are the answers:
Very good – 20,0%
Positive – 31,3%
Indifferent – 2,79%
Bad – 0,5%
Negative – 0,4%
No indication – 14%
That question was not asked to the patients who had cesarean section.
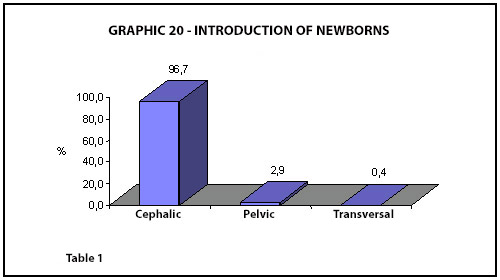
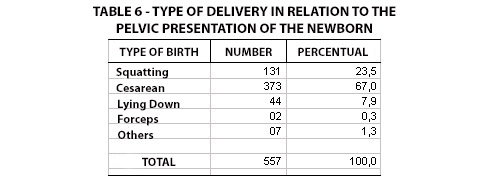
Breech Deliveries
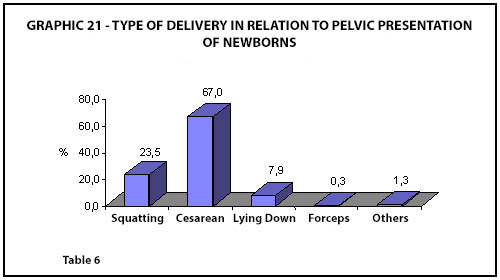
They occurred to 2,9% of the population. The indication breech presentation in primiparous woman = cesarean operation has been followed by almost all the medical population except for a few patients.
Thus 67% of this population had C-section delivery, 24% squatting position delivery, and there have been 2 forceps deliveries in 557 cases.
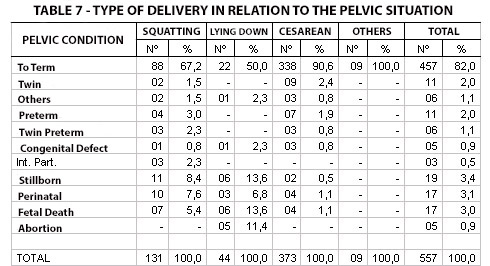
BREECH DELIVERIES:
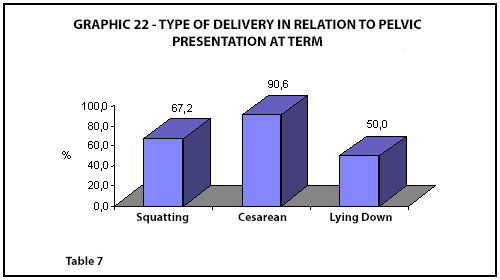
82% mature
3% twins – 1% premature
2% premature
1% congenital defect
10% mortality rate
BREECH IN SQUATTING POSITION:
70% mature
6% twins – 2% premature
3% premature
1% congenital defect
24% mortality rate
BREECH IN SUPINE POSITION:
50% mature
2% congenital defect
37% mortality rate
BREECH IN C-SECTION:
91% mature
2% twins – 1% premature
2% premature
1% congenital defect
7% mortality rate
My comments about the above data is: they are isolated valuable but they restrain comparison because they are not divided into homogeneous groups. In general words we can say that mortality in this group is related to prematurity.
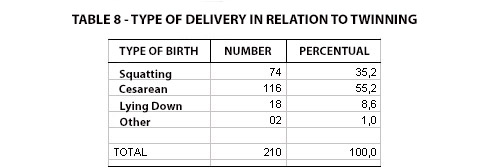
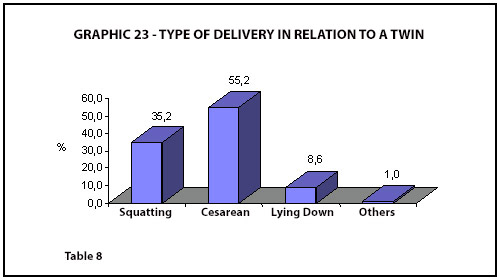
Twin Deliveries
They occurred to 1,07% of the population – 210 cases. From this group 55% were born through cesarean section, 35% in the squatting position, and 9% in the supine position.
Twins: 76% mature, 19,5% premature, 5% mortality
Twins in the squatting position: 73% mature, 21,6% premature, 5,4% mortality
Twins in the supine position: 66,5% mature, 22,2% premature, 11,1% mortality
Twins through C-section: 79,3% mature, 18,1% premature, 2,5% mortality
Newborns Weight
Over 2.500 grams – 9,1%
Under 2.500 grams – 5,2%
No indication – 3,6%
Putting these data in Battaglia and Lubchenko’s risk graphic and associating them with natimortality we see that the group found follows the patern and that there are high points which are related to prematurity.